
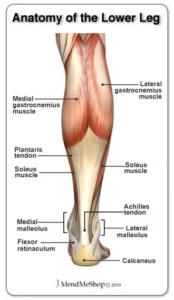
The Achilles tendon connects the gastrocnemius, soleus, and plantaris muscles to the calcaneus. It is the largest and strongest tendon in the body, enabling foot plantarflexion, which is essential for walking, running, and jumping. However, overuse, degeneration, or repetitive stress can lead to Achilles tendinopathy. Pain, stiffness, swelling, or reduced tendon function typically characterize this condition.
Tendinopathy is an umbrella term for pathology that includes acute inflammatory changes or “tendonitis” and chronic degenerative changes or “tendinosis.” The condition is especially common in the athletic and active populations, with a lifetime prevalence of 24%, and occurs more frequently in males than females at a ratio of 3.5:1, remarkably increasing incidence in recreational athletes over 25 years old.
What Causes Achilles Tendinopathy?
Achilles tendonitis is typically caused by overuse and mechanical overload of a tendon. This condition often occurs in mostly sedentary individuals who suddenly increase repetitive mechanical load, known as “weekend warriors.” An imbalance in gastrocnemius-soleus muscle strength and flexibility compared to Achilles tendon strength and flexibility can also lead to micro-tearing of the tendon, resulting in an acute inflammatory response that causes pain and swelling. Finally, repetitive microtrauma and prolonged inflammation may prevent the cell matrix from adequately synthesizing matrix proteins to repair the micro-tearing, leading to degradation and maladaptive remodeling of the tendon.
This process can develop into tendinosis, causing a weaker, less pliable tendon. The body’s ability to heal tendon micro-tearing and control acute inflammation depends on the blood supply to the tendon. The Achilles tendon receives its blood supply at the proximal and distal sections from the posterior tibial artery and its midsection from the peroneal artery. The distal 2-6 cm of the midsection of the tendon is known as the “watershed zone,” which receives the least amount of blood supply and is highly susceptible to tendinopathy and rupture due to its hypovascular nature.
Comorbid conditions such as diabetes, heart failure, and peripheral vascular disease can further reduce blood supply to the tendon, increasing the risk of injury. Additional intrinsic risk factors, including advanced age, male sex, lateral ankle instability, and extrinsic risk factors such as obesity, fluoroquinolone use, prolonged corticosteroid use, and a sedentary lifestyle, can also increase the risk of developing Achilles tendinopathy.
Diagnosis of Achilles Tendinopathy
The diagnosis of Achilles tendinopathy is primarily clinical based on symptoms of pain at the insertion of the Achilles onto the calcaneus (insertional tendinopathy) or at the proximal to mid-portion of the Achilles (non-insertional tendinopathy), as well as a thorough physical exam. Exam maneuvers such as the arc sign and Royal London Hospital test, along with palpation of nodules and assessment of tendon thickening or symmetry, can aid in confirming tendinopathy.
Ultrasound is also beneficial in the early stages of tendinitis due to its sensitivity in detecting early enthesitis. Plain radiographs help identify tendon calcifications, while MRI provides valuable information regarding tendon thickness, with abnormal Achilles thickness measured as greater than 7mm.
Eccentric Strengthening for Conservative Management of Achilles Tendinopathy
Conservative management of Achilles tendinopathy involves a multifaceted rehabilitation approach focused on strengthening, stretching, and improving the range of motion of the tendon. Eccentric strengthening of the Achilles is a key treatment strategy shown to improve pain and function in patients with Achilles tendinopathy. This training involves assisting the affected ankle into maximum plantar flexion followed by slow, unassisted, controlled movement into end-range dorsiflexion, known as an “eccentric drop.”
Compared to concentric and isometric training, eccentric training allows for the most force production relative to the energy cost required, resulting in muscle/tendon lengthening as resistance becomes greater than the force generated by the muscle/tendon. Notably, because of the high force production, eccentric exercises can cause acute inflammation and exacerbate the symptoms of Achilles tendinitis, making this training more suitable for tendinosis than tendinitis.
Alfredson developed a widely accepted protocol in 1998 for eccentric Achilles strengthening consisting of a 12-week program using three sets of 15 reps of unilateral straight and bent leg eccentric drops twice daily for 180 reps, 7 days per week. The Alfredson protocol found significant decreases in pain and increases in calf strength at the end of the 12 weeks in all subjects tested6. A 2001 study by Mafi et al. compared eccentric calf training to concentric training in patients with chronic Achilles tendinosis and found a clinically significant improvement in pain and function in the eccentric group compared to the concentric group at 12 weeks7. A 2017 study by Habets et al. compared the Alfredson protocol with the Silbernagel method, a 12-week program utilizing a combination of concentric, eccentric, and plyometric training for Achilles rehabilitation and found clinically significant improvements in pain and function in both groups up to 1-year follow-up with no clinically significant difference in the programs, further underscoring the importance of eccentric tendon strengthening.
Overall, eccentric training is a valuable rehabilitation tool for managing Achilles tendinopathy. A person can implement this training right at home and cheaply. For these reasons, patients should consider incorporating it into their rehabilitation programs to reduce pain and improve function.
References
- Pedowitz D, Kirwan G. Achilles tendon ruptures. Curr Rev Musculoskelet Med. 2013 Dec;6(4):285-93. doi: 10.1007/s12178-013-9185-8. PMID: 24151122; PMCID: PMC4094105.
- Lopez RG, Jung HG. Achilles tendinosis: treatment options. Clin Orthop Surg. 2015 Mar;7(1):1-7. doi: 10.4055/cios.2015.7.1.1. Epub 2015 Feb 10. PMID: 25729512; PMCID: PMC4329521.
- Chen, T.M., Rozen, W.M., Pan, W.-r., Ashton, M.W., Richardson, M.D. and Taylor, G.I. (2009), The arterial anatomy of the Achilles tendon: Anatomical study and clinical implications. Clin. Anat., 22: 377-385. https://doi.org/0.1002/ca.20758
- Wong M, Jardaly AH, Kiel J. Anatomy, Bony Pelvis, and Lower Limb: Achilles Tendon. [Updated 2023 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499917/
- Jayaseelan DJ, Mischke JJ, Strazzulla RL. Eccentric Exercise for Achilles Tendinopathy: A Narrative Review and Clinical Decision-Making Considerations. J Funct Morphol Kinesiol. 2019 Jun 5;4(2):34. doi: 10.3390/jfmk4020034. PMID: 33467349; PMCID: PMC7739229.
- Alfredson H, Pietilä T, Jonsson P, Lorentzon R. Heavy-load eccentric calf muscle training for treating chronic Achilles tendinosis. Am J Sports Med. 1998 May-Jun;26(3):360-6. doi: 10.1177/03635465980260030301. PMID: 9617396.
- Mafi N, Lorentzon R, Alfredson H. Superior short-term results with eccentric calf muscle training compared to concentric training in a randomized prospective multicenter study on patients with chronic Achilles tendinosis. Knee Surg Sports Traumatol Arthrosc. 2001;9(1):42-7. doi: 10.1007/s001670000148. PMID: 11269583.
- Habets B, van Cingel REH, Backx FJG, Huisstede BMA. Alfredson versus Silbernagel exercise therapy in chronic midportion Achilles tendinopathy: study protocol for a randomized controlled trial. BMC Musculoskelet Disord. 2017 Jul 11;18(1):296. doi: 10.1186/s12891-017-1656-4. PMID: 28693535; PMCID: PMC5504829.




